Sample Level 2 Recovery House Application from the Fletcher Group
**Disclaimer:** The following content was written by the Fletcher Group (https://www.fletchergroup.org) and is provided for example purposes only. For technical assistance and training tailored to recovery homes, we encourage you to reach out to the Fletcher Group directly. We are grateful for their expertise and appreciate the opportunity to share these valuable templates with our audience.
--------------------------------
Sample Handbook for Rural Recovery Residences (Level II)
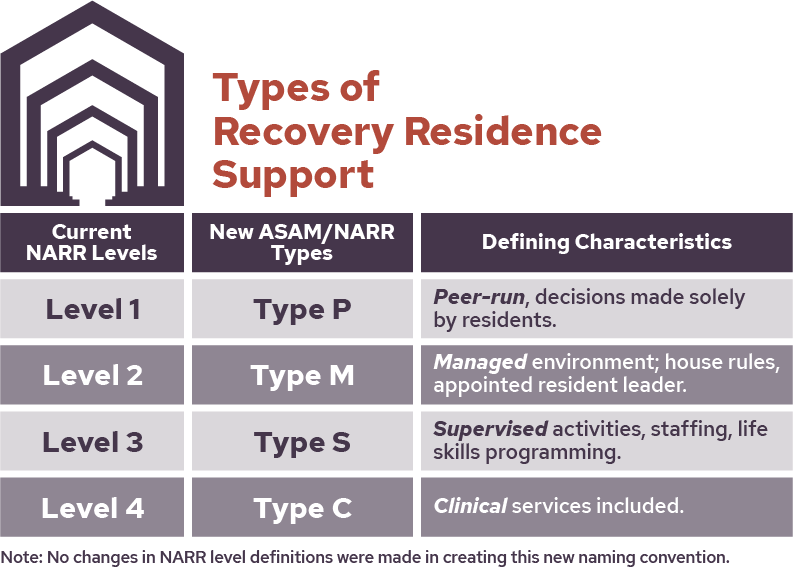
This Recovery Residence offers Level II support in a monitored facility that has house rules to provide structure and includes peer run groups, drug testing, house meetings, and participation in treatment services and/or self-help meetings. Our residence is provided in a [single family home or apartment building] located at [enter address here]. It is democratically run based on a handbook and policies & procedures. We have a paid House Manager that helps manage the house and provide guidance and support. Residents are encouraged to also participate in available recovery support services in the community.
The [enter Recovery Residence name here] requires that its residents have been in recovery for at least [enter required length of sobriety] before moving into the residence. In addition, all residents are expected to commit to providing peer support for other residents,participate in recovery planning with peers and/or community supports such as outpatient counseling and/or self-help groups and confirm that recovering in a housing environment with a House Manager and Peer Support as opposed to a more intensive treatment environment is their preference.
|
Resident Evaluation/Application |
||||||||||||||
|
Peer: |
Today's Date: |
Time: |
||||||||||||
|
Desired Move-in Date: |
Reason for Move: |
|
||||||||||||
|
Applicant Name: |
|
|
||||||||||||
|
Date of Birth: |
Phone: |
|
||||||||||||
|
Current Address: |
|
|
||||||||||||
|
City: |
State: |
Zip Code: |
||||||||||||
|
Own or Rent: |
Monthly Payment or Rent: |
How Long at this address? |
||||||||||||
|
Previous Address: |
|
|
||||||||||||
|
City: |
State: |
Zip Code: |
||||||||||||
|
Own or Rent: |
Monthly Payment or Rent: |
How Long at this address? |
||||||||||||
|
Where have you lived for the past 6 Months: |
||||||||||||||
|
|
Identification: |
|
||||||||||||
|
☐Valid State I.D. |
☐Valid Driver's License |
☐Social Security Card |
||||||||||||
|
☐Birth Certificate |
☐Convicted of a Violent Crime? |
☐Convicted of a Sexual Offense? |
||||||||||||
|
☐SNAP Benefits? |
|
|
||||||||||||
|
|
Marital Status |
|
||||||||||||
|
Married |
Separated |
Divorced |
||||||||||||
|
Widowed |
Registered Partnership |
|
||||||||||||
|
Do you have Children: ☐Yes ☐ No |
If yes, who is caring for them: |
|||||||||||||
|
Level of Education: |
☐Veteran? |
☐Pregnant? |
||||||||||||
|
Who referred you to us? |
|
|
||||||||||||
|
Recovery and Substance Use History |
||||||||||||||
|
Have you been a resident of the [residence name] before? |
||||||||||||||
|
☐Yes ☐ No If Yes When: |
When is the last time you used drugs? |
|||||||||||||
|
Have you sought services for a substance use disorder in the past? ☐Yes ☐No |
||||||||||||||
|
|
If yes, please list all: |
|
||||||||||||
|
Where: |
When: |
Length of Stay: |
||||||||||||
|
Where: |
When: |
Length of Stay: |
||||||||||||
|
Where: |
When: |
Length of Stay: |
||||||||||||
|
Substance Use History: |
||||||||||||||
|
Drug of use: |
Last Use: |
How Much: |
Method: |
|||||||||||
|
Drug of use: |
Last Use: |
How Much: |
Method: |
|||||||||||
|
Drug of use: |
Last Use |
How Much: |
Method: |
|||||||||||
|
Alcohol Use ☐Yes ☐ No |
If Yes, How Much: |
How Often: |
||||||||||||
|
Probation Parole/Court/Legal Issues |
||||||||||||||
|
Pending Charges or Legal Issues: ☐Yes ☐No |
If yes, please explain: |
|||||||||||||
|
|
|
|
||||||||||||
|
|
|
|
||||||||||||
|
Upcoming Court Dates: ☐Yes ☐ No |
If yes, please explain: |
|||||||||||||
|
Do you report to a Probation Officer ☐Yes ☐No |
Name/Phone: |
|||||||||||||
|
Felony Conviction in the past 3yrs: ☐Yes ☐No |
If yes, please list: |
|||||||||||||
|
Emergency Contact and Health Information |
||||||||||||||
|
Emergency Contact: |
||||||||||||||
|
Relation: |
Parent ☐ |
Spouse ☐ |
Sibling ☐ |
Friend ☐ |
Other ☐ |
|||||||||
|
Address: |
Phone Number: |
|||||||||||||
|
Please List any Medications you are currently taking: |
||||||||||||||
|
|
|
How Long: |
||||||||||||
|
Mental Health Symptoms or Conditions: ☐Yes ☐ No – If yes, please explain? |
||||||||||||||
|
Have you attempted Suicide in the past: ☐Yes ☐No |
If yes, how many times? |
|||||||||||||
|
Did you have a specific plan? |
||||||||||||||
|
Were you under the influence at the time:☐Yes ☐No |
When was your last attempt? |
|||||||||||||
|
Employment/Income |
||||||||||||||
|
What is your source of income? |
||||||||||||||
|
Amount per month: |
||||||||||||||
|
Employer (if applicable): |
||||||||||||||
|
Length of time on job (if applicable): |
||||||||||||||
|
Do you have a savings account? |
||||||||||||||
|
Do you have debts? If so, what do you pay monthly? |
||||||||||||||
Here is the full link to the Handbook.